“Radial-sided wrist pain is a common patient complaint that can have a dramatic effect on the patient’s productivity at work, sporting or artistic pursuits, and activities of daily living.” (1). When working in the hand clinic, certainly the most common diagnosis besides the trigger finger, the basilar joint arthritis, carpal tunnel syndrome, is de Quervain’s tenosynovitis.
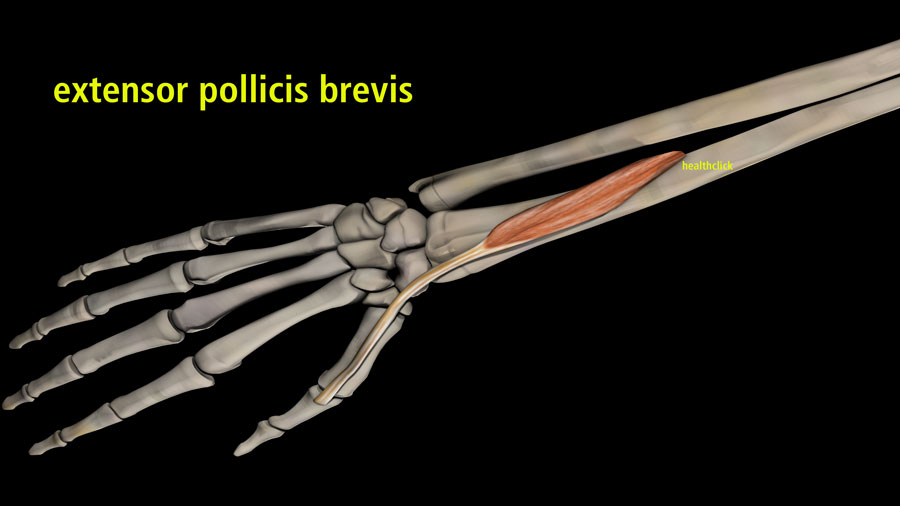
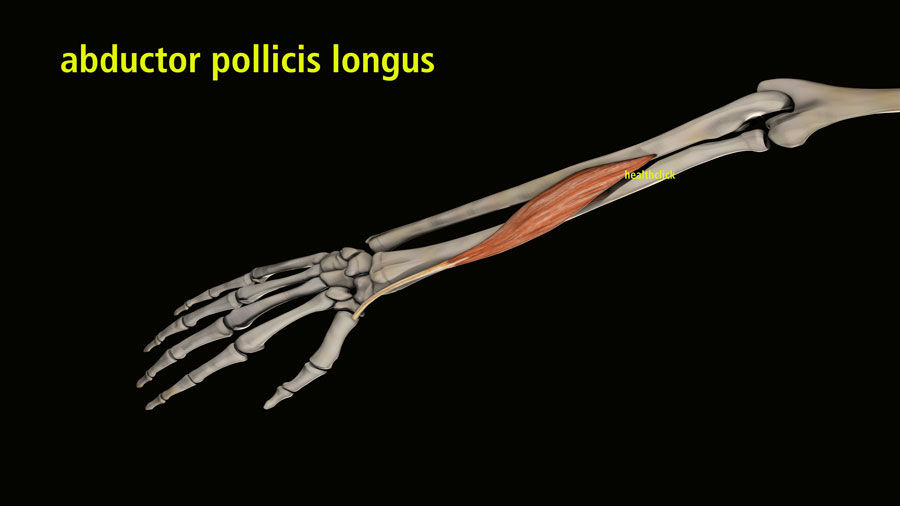
Comprised of the two tendons that pass through the first dorsal compartment is the abductor pollicis longus and the extensor pollicis brevis. I call it the cousin to trigger finger, where you have an inflammation of the extensor sheath that passes through that in a sense inflames and enlarges. It causes friction at the first dorsal compartment and is quite painful. Suppose you have one option to treat this common problem. In that case, you certainly want to use any bracing system or splinting system that will incorporate limitations of the thumb, allowing free motion at the IP joint that mobilizes the wrist and the MP of the thumb. The reason for this is this prevents that tendon from going back and forth underneath that particular sheath, causing that friction to exist.
“While the exact cause of de Quervain tenosynovitis is unclear, it has been attributed to myxoid degeneration with fibrous tissue deposits and increased vascularity rather than acute inflammation of the synovial lining.”
De Quervain Tenosynovitis
In early-stage cases, it’s typically nonsteroidal anti-inflammatories with splinting. If you’re going to treat them in the clinic, certainly any of your modalities that increase blood flow to that area is a massage. Some people will perform isometrics there to prevent any atrophy. I find that to be optional. We’ll do very well in conservative management.
From the standpoint of surgical management, though, this is also very similar to trigger finger; they will have an injection of corticosteroid. If those all fail, the options are to release that first dorsal compartment. That allows for freedom of the inflamed tendon to pass through without promoting that inflammation or irritation.
In that case, you’re now going to add to your treatment protocol edema reduction in that area. You’re still going to use modalities, massage, and soft tissue mobilization. Also, in this perspective, you will consider scar management, which, typically, scar gel is ideal. Ultrasound is beneficial for this condition because it is so superficial.
Learn more about De Quervain Tenosynovitis in our All Access Annual Subscription for $189/year.
The video in this blog is referenced from the concussion rehab continuing education course, Functional Management of the Elbow, the Wrist, and the Hand. This online course is included in our all-access annual subscription. Learn from this multidisciplinary approach, updated therapeutic management techniques and medical practices for post-traumatic headaches, and how to properly assess and treat migraines, cervicogenic/tension headaches, occipital neuralgia, and medication overuse headaches in this comprehensive course concussions.
The Best Value for Video Continuing Education
Other courses within this subscription that will assist with better management of upper extremity injuries include:
Injury Prevention and Optimal mechanics in the Throwing Athlete
Critical Analysis and Treatment Strategies for the Complex Shoulder
Foundation Exercises for the Treatment of the Shoulder
The Science of taping: Determining Effective Techniques for Specific Diagnoses
A healthclick subscription impacts patients’ lives across the US and has empowered your colleagues to deliver better care. In 2021, our films raised over $150,000 to assist special-needs children in accessing better rehabilitation. We donated our time and resources without charge to create films that non-profit used to raise all these funds. Money that went directly to therapists and your colleagues to deliver their rehab vision to their population.
Tom Vastano – Filmmaker, healthclick
References
1. Allbrook, V. (2019). “The side of my wrist hurts”: “De Quervain”s tenosynovitis’. Australian Journal of General Practice, 48(11), 753–756. https://search.informit.org/doi/10.3316/informit.728871641057934
2. Ashraf, Muhammad Omer, and V. G. Devadoss. “Systematic review and meta-analysis on steroid injection therapy for de Quervain’s tenosynovitis in adults.” European Journal of Orthopaedic Surgery & Traumatology 24.2 (2014): 149-157.
3. Awan, Waqar Ahmed, Babur, Muhammad Naveed, and Masood, Tahir. ‘Effectiveness of Therapeutic Ultrasound with or Without Thumb Spica Splint in the Management of De Quervain’s Disease’. 1 Jan. 2017 : 691 – 697.
4. Goel R, Abzug JM. De Quervain’s Tenosynovitis: A Review of the Rehabilitative Options. HAND. 2015;10(1):1-5.
5. Orlandi, D., Corazza, A., Fabbro, E. et al. Ultrasound-guided percutaneous injection to treat de Quervain’s disease using three different techniques: a randomized controlled trial. Eur Radiol 25, 1512–1519 (2015).
6. Rocco Cavaleri, Siobhan M. Schabrun, Maxine Te, Lucy S. Chipchase, Hand therapy versus corticosteroid injections in the treatment of de Quervain’s disease: A systematic review and meta-analysis, Journal of Hand Therapy,
Volume 29, Issue 1, 2016, Pages 3-11, ISSN 0894-1130.